What are palatal expanders?
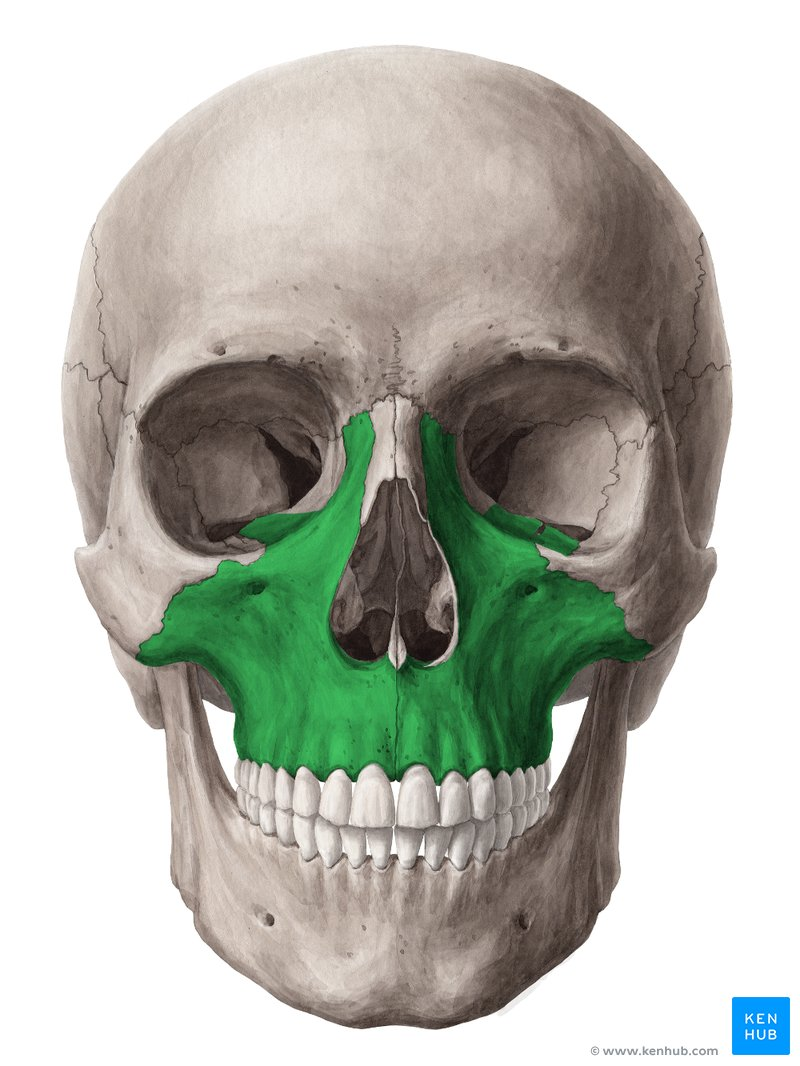
Palatal expanders are orthodontic devices that are used to widen the upper jaw (maxilla).
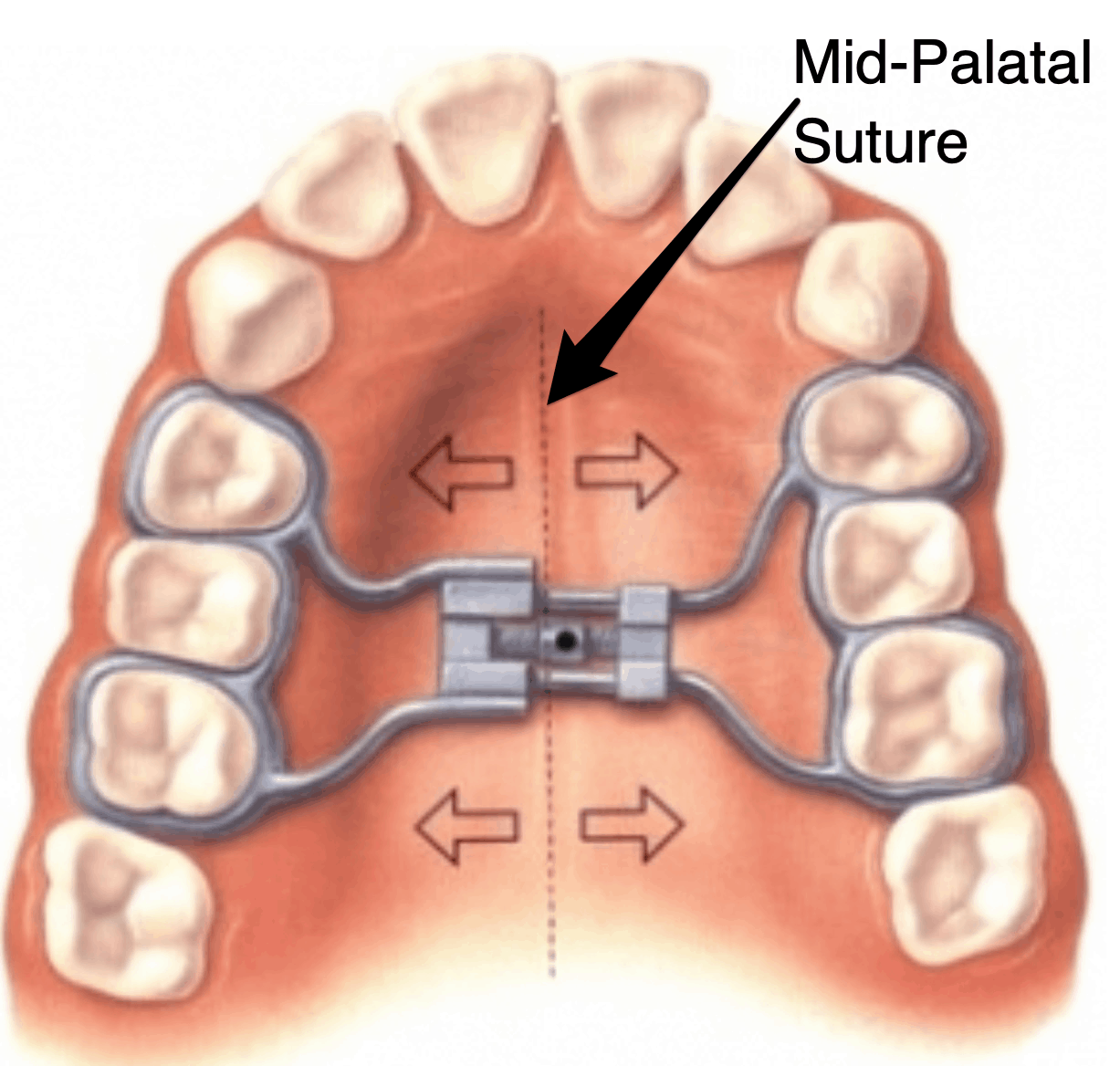
They work by applying gentle but constant force to separate the two halves of the maxilla at the midpalatal suture.
In children, the suture is still soft and flexible, which makes it easy to expand. -In adults, the suture is more fused, which requires stronger force (MSE) or surgical assistance (SARPE).
Reference: https://doi.org/10.1007/s11325-020-02140-y
Why Would Someone Need a Palatal Expander?
A palatal expander is more than just an appliance that is used to straighten teeth. It is often prescribed to address a mix of functional, health-related, and aesthetic concerns that all trace back to the width of the maxilla.
Maxillary expansion changes the way that the teeth, bones, and airway interact with each other, which has a host of functional as well as aesthetic benefits.
Dental / Orthodontic Reasons
When the maxilla is too narrow, the upper teeth may not align properly with the lower teeth or there may not be enough space to fit all teeth naturally. This creates a host of problems functionally.

● Crossbite Correction: - A narrow upper jaw can cause the upper back teeth to fit inside the lower back teeth instead of overlapping them properly. - This misalignment puts strain on the teeth, gums, and jaw joints, and can cause uneven tooth wear over time. - Expansion repositions the upper teeth outward so the bite is balanced and functional.

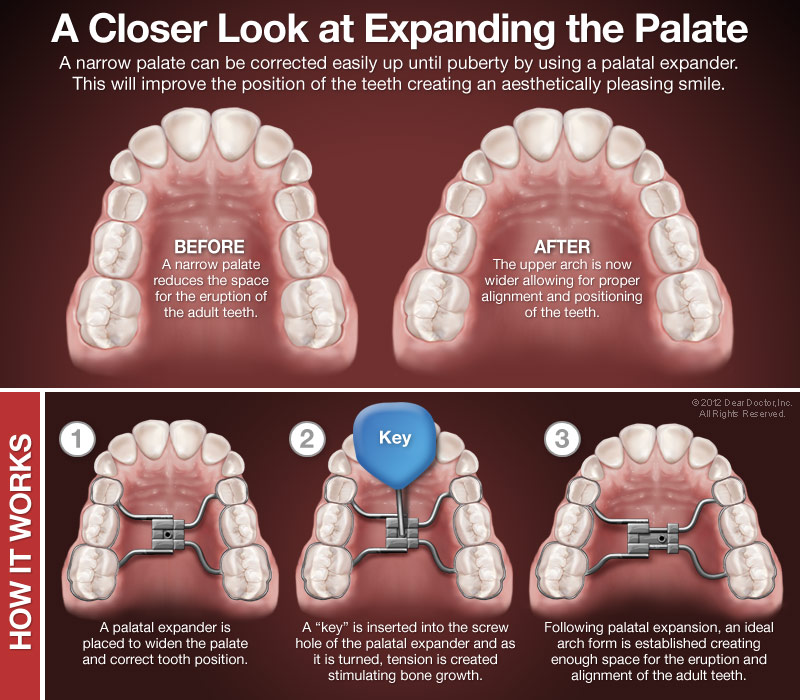
● Narrow Dental Arch: - Some people naturally have a “V-shaped” or constricted arch that makes their smile look narrow and can crowd teeth forward or backward. Ideally, one would want a “U-shaped” arch. - Expanding the palate creates a broader “U-shaped” arch, making more space for teeth to sit evenly.

● Crowding & Space Creation: - Without enough jaw width, permanent teeth may overlap, twist, or erupt out of alignment. - Expansion can create space naturally, often avoiding the need to extract healthy teeth just to make room.

● Preventive Orthodontics: - In growing children, expansion can prevent severe crowding or misalignment before all permanent teeth erupt, making later orthodontic treatment simpler and faster.
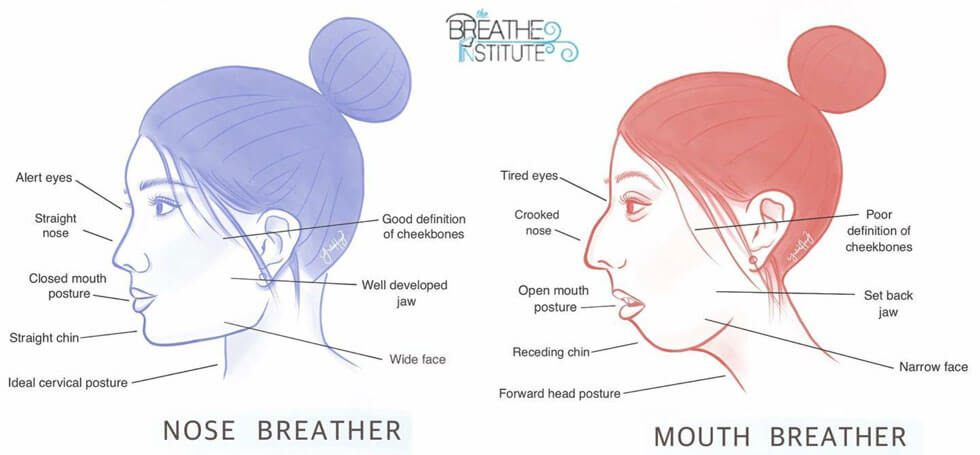
Breathing & Airway Reasons
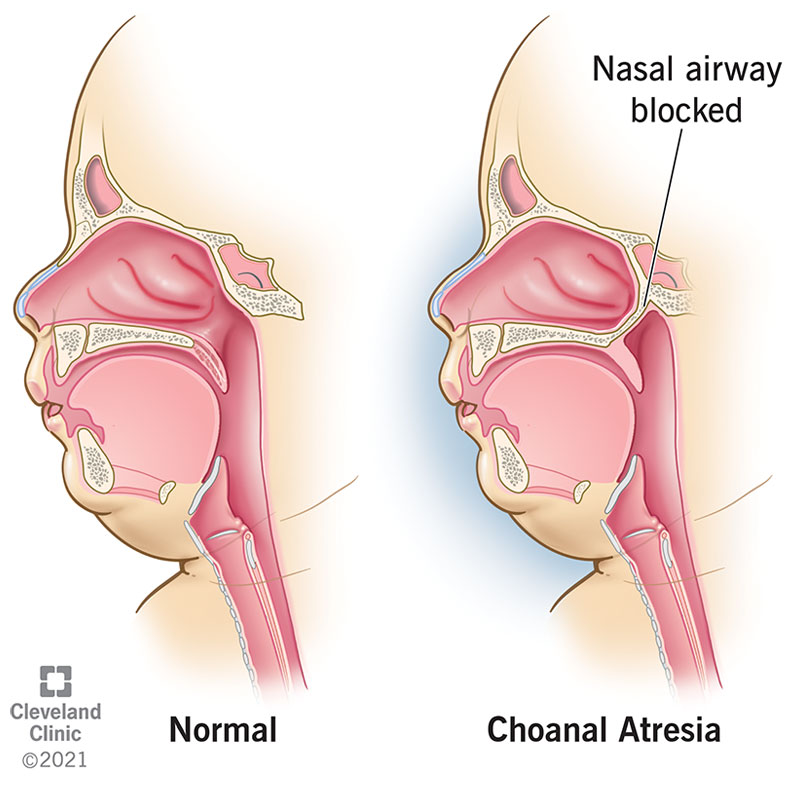
The maxilla not only holds the upper teeth but also forms the bony floor of the nasal cavity, so its width plays a key role in how much space the nasal passages have for airflow. When the maxilla is narrow, the nasal cavity can be constricted, making it harder for air to pass through. Widening the maxilla with a palatal expander increases nasal cavity volume, reduces airflow resistance, and can make nasal breathing easier and more efficient.
● Narrow Nasal Airway: - A constricted palate can lead to a smaller nasal cavity, which increases resistance to airflow. - By widening the palate, the nasal passages also expand, often improving nasal breathing.
● Chronic Mouth Breathing: - Mouth breathing can be both a symptom and a cause of jaw narrowing. - Expansion helps open the nasal airway, making it easier and more comfortable to breathe through the nose.
● Snoring & Sleep-Disordered Breathing: - In some patients, especially children, a narrow palate can contribute to snoring or mild obstructive sleep apnea. - Expansion can improve airflow at night, sometimes reducing these symptoms and improving sleep quality.

● Overall Health Impact: - Better nasal breathing can improve oxygen intake, sleep quality, focus, and even athletic performance over time.
Aesthetic Reasons
Maxillary width influences not just the smile, but the entire midface appearance. Because the maxilla forms the central foundation for key facial structures such as the cheeks, nose, and 4 upper lip, its size and position affect how full or flat your face appears.
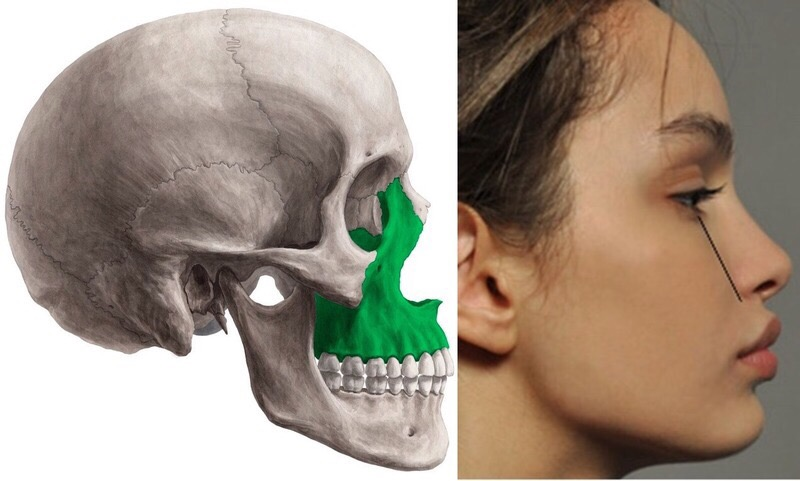
A wide and anteriorly projected maxilla contributes to an attractive smile and overall facial harmony. Conversely, a narrow or underdeveloped upper jaw can lead to a constricted smile, flattened cheeks, and a detriment to facial aesthetics.
● Narrow Smile: - A constricted arch can leave “dark spaces” at the corners of the mouth when smiling (known as buccal corridors). - Expansion broadens the arch so more teeth show, creating a fuller and more attractive smile.

● Flat or Underdeveloped Midface: - The maxilla supports the cheeks, lips, and nose. - Widening the palate can subtly improve facial harmony, support the upper lip, and give a less “collapsed” appearance.

● Youthful Facial Proportions: - Broader dental arches are often associated with a younger, more balanced facial structure, and expansion can help restore these proportions

How do they work?
Step 1 - Diagnosis & Planning
-Assessment of jaw width, bite alignment, facial profile, and airway space.
- Diagnostic tools: impressions or digital scans, intraoral and facial photographs, panoramic and cephalometric X-rays, sometimes CBCT scans for a 3D view.
- Appliance choice based on age, suture maturity, and treatment goals:
- Tooth-borne (anchored to molars/premolars) 5 - Bone-borne (MSE/MARPE) (anchored with mini-implants in the palate)
- Surgically Assisted (SARPE) (used when sutures are fused in mature adults)
At this stage, the orthodontist will carefully determine whether your midpalatal suture can be opened with orthodontic force alone or whether surgical help is needed. They will also consider functional needs like correcting a crossbite, creating space for crowded teeth, or improving airway function. Planning is highly individualized, and this step is the foundation for a safe and predictable expansion.
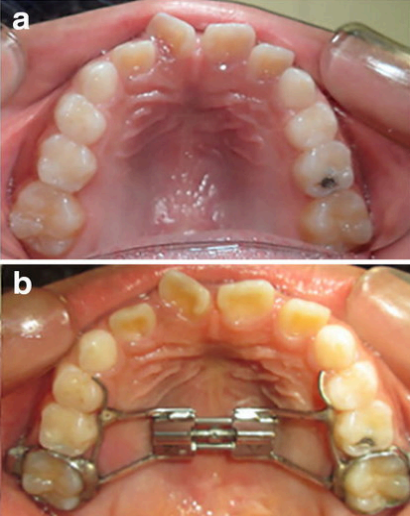
Step 2 - Fitting
The fitting appointment is often straightforward for tooth-borne devices, but bone-borne expanders require a brief procedure to place the implants. The orthodontist ensures the appliance sits snugly without rocking and provides cleaning instructions, since food can easily get trapped around the hardware.
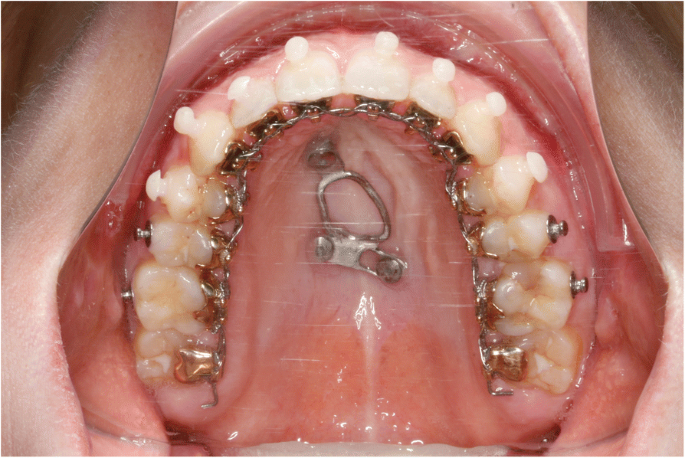
- Tooth-borne: Metal bands cemented to selected molars/premolars, connected by a rigid expansion screw in the middle of the palate.
- Bone-borne (MSE/MARPE): tiny titanium implants (TADs) placed in the hard palate under local anesthesia, with the expander anchored directly to bone.
- Surgically Assisted (SARPE): combines both teeth and bone anchorage for greater stability. Appliance adjusted for comfort and checked to avoid gum or tongue irritation.

Step 3 – Latency Period (sometimes)
This short waiting period is mainly for comfort. It gives the palate’s connective tissues a chance to adapt before active force is applied. It’s not mandatory but can reduce early discomfort, especially in adults or when using more rigid bone-borne appliances.
- Duration: usually 1-2 days for bone-borne expanders - Purpose: allows for tissues to adapt and for initial inflammation to subside
- Often skipped in children, where sutures are more pliable.
Step 4 – Activation (Turning the Screw)
Activation is where the real movement begins. The screw in the center of the appliance gradually pushes the left and right halves of your upper jaw apart. The forces are steady and controlled to avoid trauma, and the orthodontist may adjust the schedule based on your age, bone density, and treatment goals.
- The standard rate is 1-2 turns per day (0.25mm for each turn)
- Turns made with a small key inserted into the screw’s hole - Common sensations are pressure in teeth, roof of the mouth, nasal bridge, or cheekbones, and occasional mild headaches are common
Step 5 – Force Transmission
- Tooth-borne: force moves from the appliance → teeth → alveolar bone → palatal bone → midpalatal suture. More likely to tip teeth outward if not monitored.
- Bone-borne: force moves from appliance → implants → palatal bone → suture. Produces more skeletal change and less tooth movement.
The difference here is structural: tooth-borne expanders rely on teeth as “handles,” which can cause dental side effects, while bone-borne expanders bypass the teeth entirely, applying force directly to the skeletal structure.

Step 6 – Sutural Separation
When the suture begins to part, the first visible clue is often that space between the two central incisors.
This gap is temporary: it will often close naturally during retention or with braces, but it’s an important indicator of real skeletal change rather than just tooth movement.
- Opening starts anteriorly, and progresses posteriorly
- This often creates a visible midline gap between the upper front teeth, which is a sign that the skeletal separation is a success.
Step 7 – Expansion Phase
The expansion phase is short compared to retention, but it’s critical. Your orthodontist will monitor the progress regularly, sometimes adjusting the turning schedule to prevent overexpansion or dental strain.
- The typical goal is 6-10mm of widening
- This takes usually between 1 to 3 weeks of turning. The gap between the suture halves is initially filled with soft connective tissue

Step 8 – Retention Phase
This is the “healing” stage.
The connective tissue in the gap slowly converts into new bone through a process called ossification.
Stability is the priority here: the expander acts as an internal splint to hold the two halves of the palate in place until the bone is fully mature.
- The appliance remains in place without turning for 3-12 months
- This allows bone to mineralize and harden in the new position
- Early removal risks relapse, where the maxilla will narrow again
Step 9 – Appliance Removal
Removal is quick and painless compared to the fitting. The next phase of treatment will keep the width stable and continue to align your teeth into the new, broader arch.
Long-term retention is important because even well-healed expansion can relapse slightly without maintenance.
- Performed once imaging or clinical assessment condoms bone stability
- Retainer, braces, or clear aligners are used to maintain the results
- This is sometimes followed by additional orthodontic work to refine the bite

Pros
● Corrects crossbite and prevents crowding if the palate is expanded early. In many cases, this is preferable for aesthetics.
● Enhances facial aesthetics by preventing mouthbreathing (opposite of mewing) and improving airways.
There is strong literature supporting the idea that it impacts maxilla and mandible growth:
“Results suggest that solving maxillary hypoplasia and, therefore, premature contacts are likely to have allowed mandibular repositioning and condylar growth. RME is a safe and effective solution that can substantially improve maxillary and mandibular symmetry in growing patients affected by JIA with TMJ involvement.”
Reference: https://pmc.ncbi.nlm.nih.gov/articles/PMC7230922/
● It is generally a cheap and cost-effective method of expanding the maxilla and widening the skull in some cases, as seen below:

Cons
● With post-pubertal development, the suture within the maxilla begins to fuse, resulting in non-surgical palatal expanders being required. If one were to deploy a non-surgical palatal expander on a developed person, it may result in tooth tipping (exactly what it sounds like)
